06 Designing the Video Consultation
Zero-learning-curve entry. Receive link, tap, in the call. No app download, no account creation, no permissions dialogs. Every barrier removed between the patient and the clinician.
Minimal on-screen controls for the patient: clinician's face, end call, mute. That's it. Nothing else on screen to confuse, distract, or require explanation.
Clinician side designed for speed. Patient video, assessment questions, documentation fields, and patient record all visible simultaneously. The asymmetry was intentional - the patient sees simplicity, the clinician sees everything they need to work efficiently.
Intentional Asymmetry
Patient Side
3 elements total. Nothing to learn.
Clinician Side
Information-dense. Designed for clinical speed.
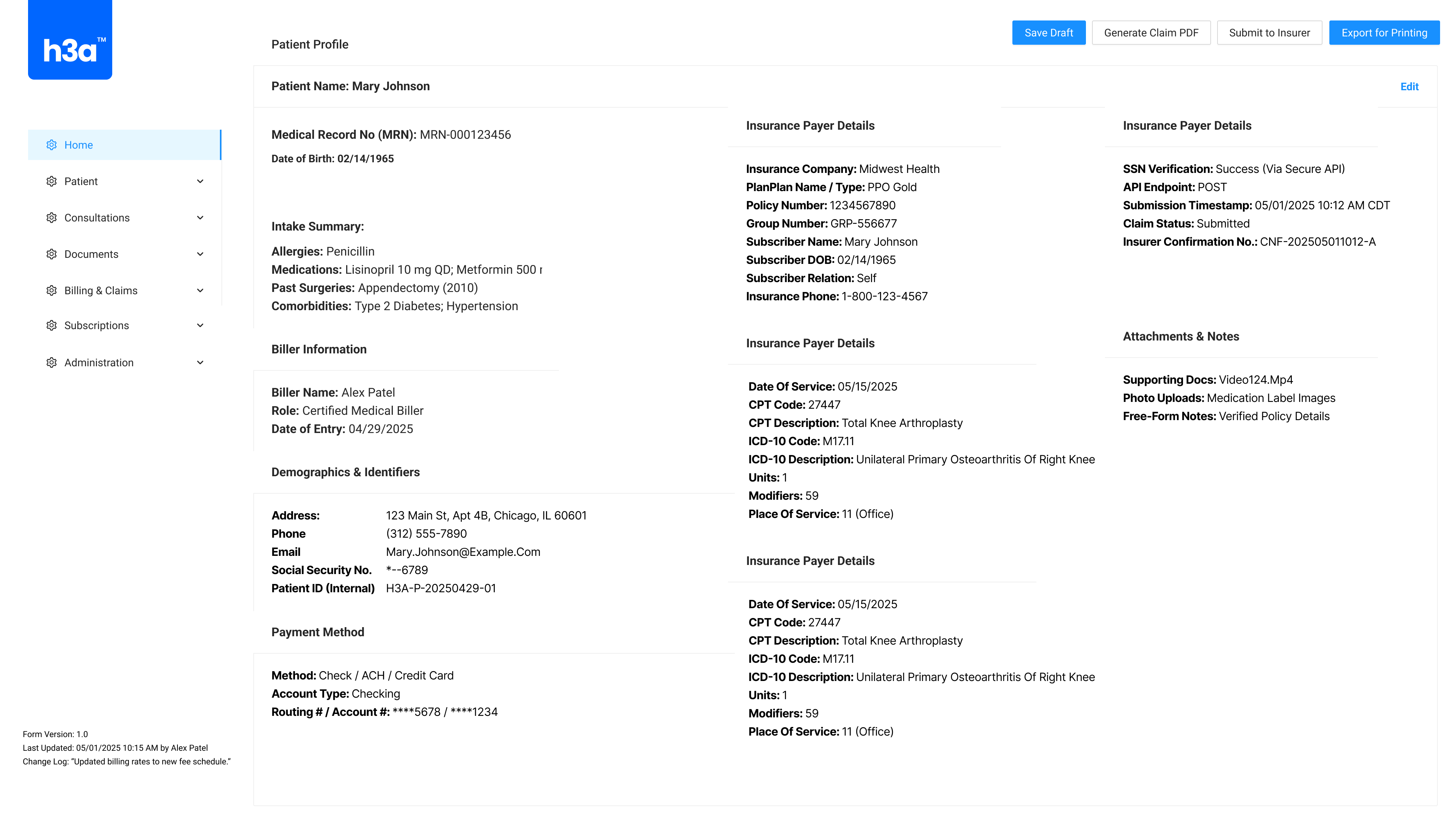
Video Consultation - Clinician View

Patient video, medical record, notes, and participant roster visible simultaneously. Click to enlarge.